Implant breast reconstruction is a common option for restoring breast shape and volume after a mastectomy. Using saline or silicone implants, reconstruction can be performed in stages or as a direct-to-implant procedure, depending on a patient's anatomy and treatment plan. Dr. Neil Tanna offers advanced implant reconstruction in New York with a personalized approach designed to achieve safe, natural-looking results.


Types of Implant Breast Reconstruction
- Expander-implant breast reconstruction
- Direct-to-implant breast reconstruction
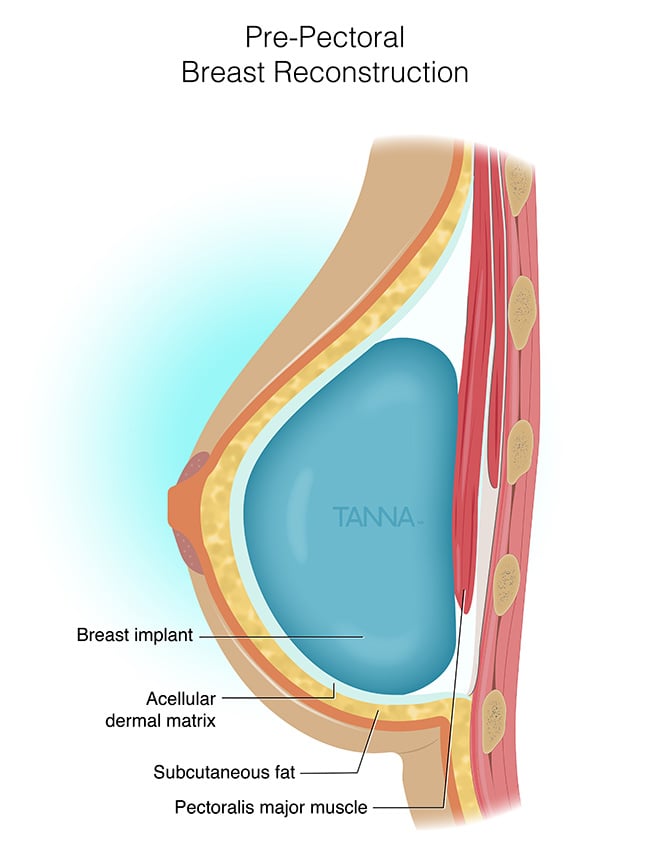
- Pre-pectoral breast reconstruction
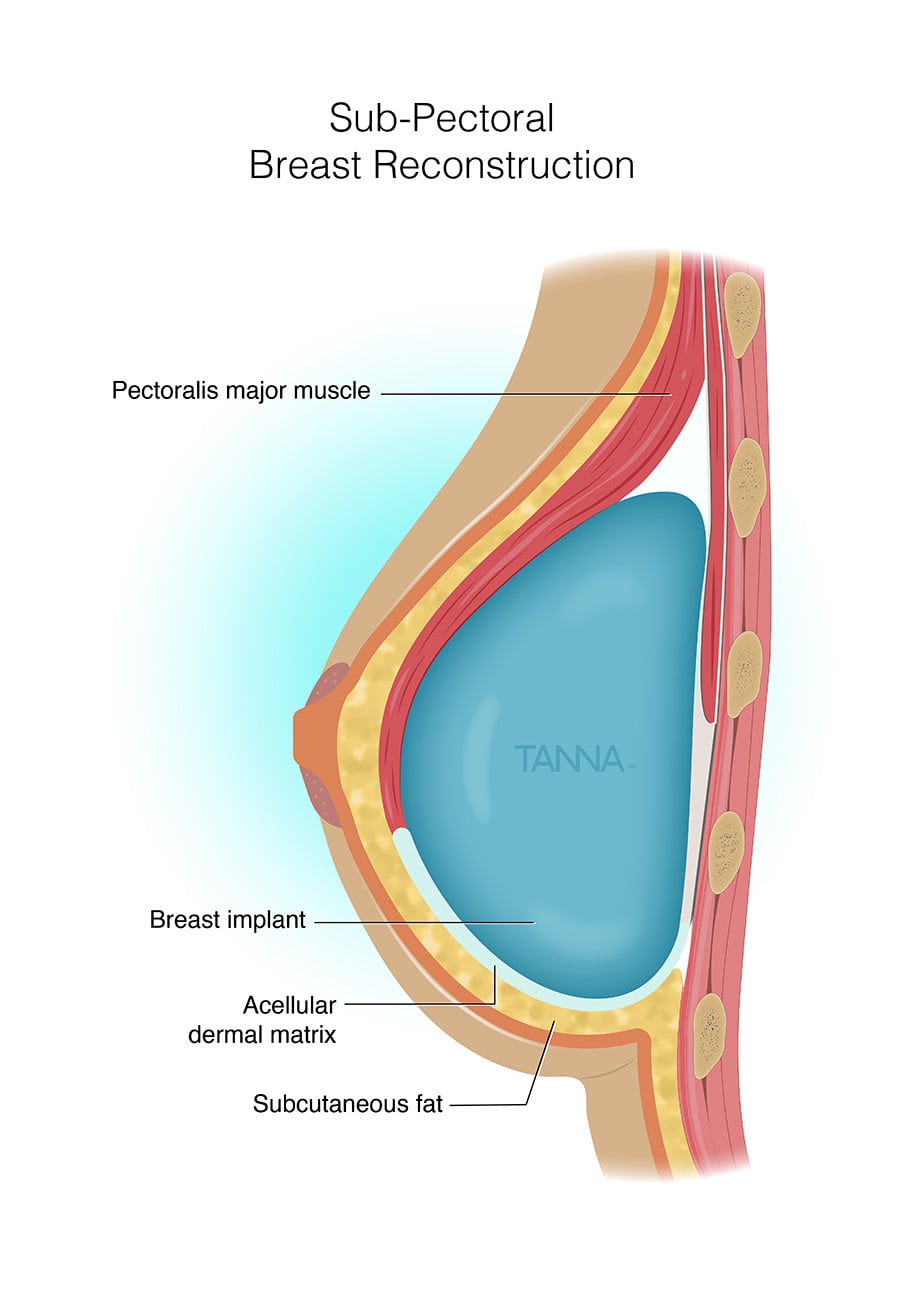
In these techniques, acellular dermal matrix (ADM) (a supportive medical product for soft tissue reconstruction) may be required. It is important to consult with Dr. Tanna to decide which implant and reconstruction operation will be most appropriate for your unique condition.