Poland syndrome is a congenital disorder that affects chest and breast development on one side of the body.


Poland Syndrome Reconstructive Surgery
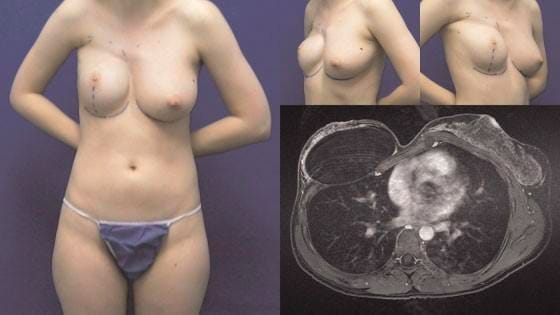
Many of the deformities with Poland syndrome can be corrected with reconstructive surgery. We offer corrective procedures such as implant-based or autologous breast reconstruction, chest wall implants, and nipple-areola reconstruction. Each of these procedures can help restore a more symmetric and natural look to the side affected by Poland’s syndrome.
For breast reconstruction, we offer the latest in microsurgical flap reconstruction, including DIEP, SIEA, TUG, and PAP flaps. We recognize that women with Poland syndrome may have problems with muscle development, and as such, we try to avoid procedures such as TRAM or Latissimus Dorsi flaps that remove muscle as well as fat. During your visit, Dr. Tanna will work with you to design a breast reconstruction plan that’s personalized to match your experience with Poland syndrome.